Malaria
Table of Contents
Introduction
Malaria is a life-threatening disease caused by plasmodium parasites that are transmitted to people through the bites of infected female Anopheles mosquitoes. According to the World Health Organization, there were an estimated 241 million cases of malaria worldwide in 2020, and about 627,000 deaths. Around 90% of all malaria cases and deaths occur in Africa south of the Sahara desert. Malaria is preventable and curable if promptly diagnosed and adequately treated.
Symptoms
The most common symptoms of malaria include:
- Fever
- Chills
- Headache
- Muscle aches
- Tiredness
- Nausea
- Vomiting and diarrhea.
Malaria symptoms typically appear 10-15 days after an infective mosquito bite. The time between the infective bite and symptoms is shortest with P. falciparum infection and longer with P. malariae. If drugs are not available, symptoms occur in cycles that last 2-3 days at a time. In P. vivax and P. ovale infections, relapses may occur weeks or months after the first infection.
Causes & Transmission
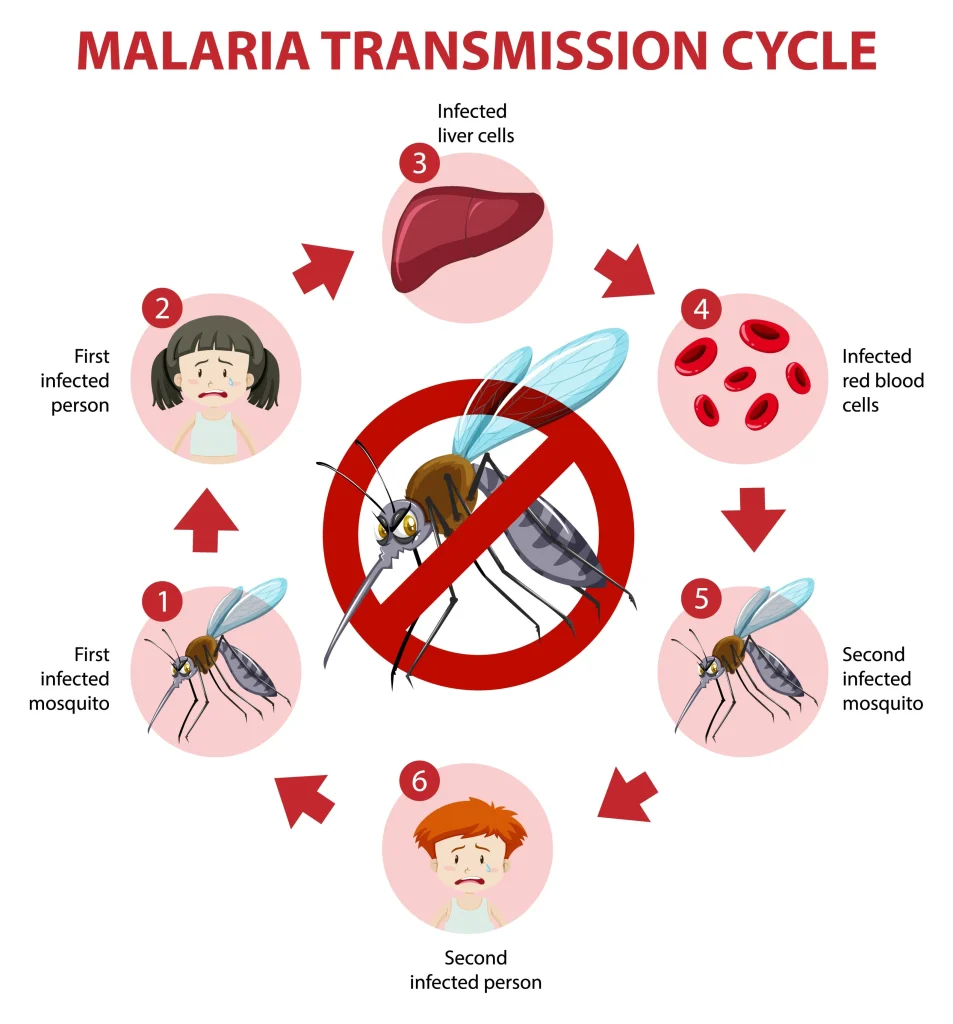
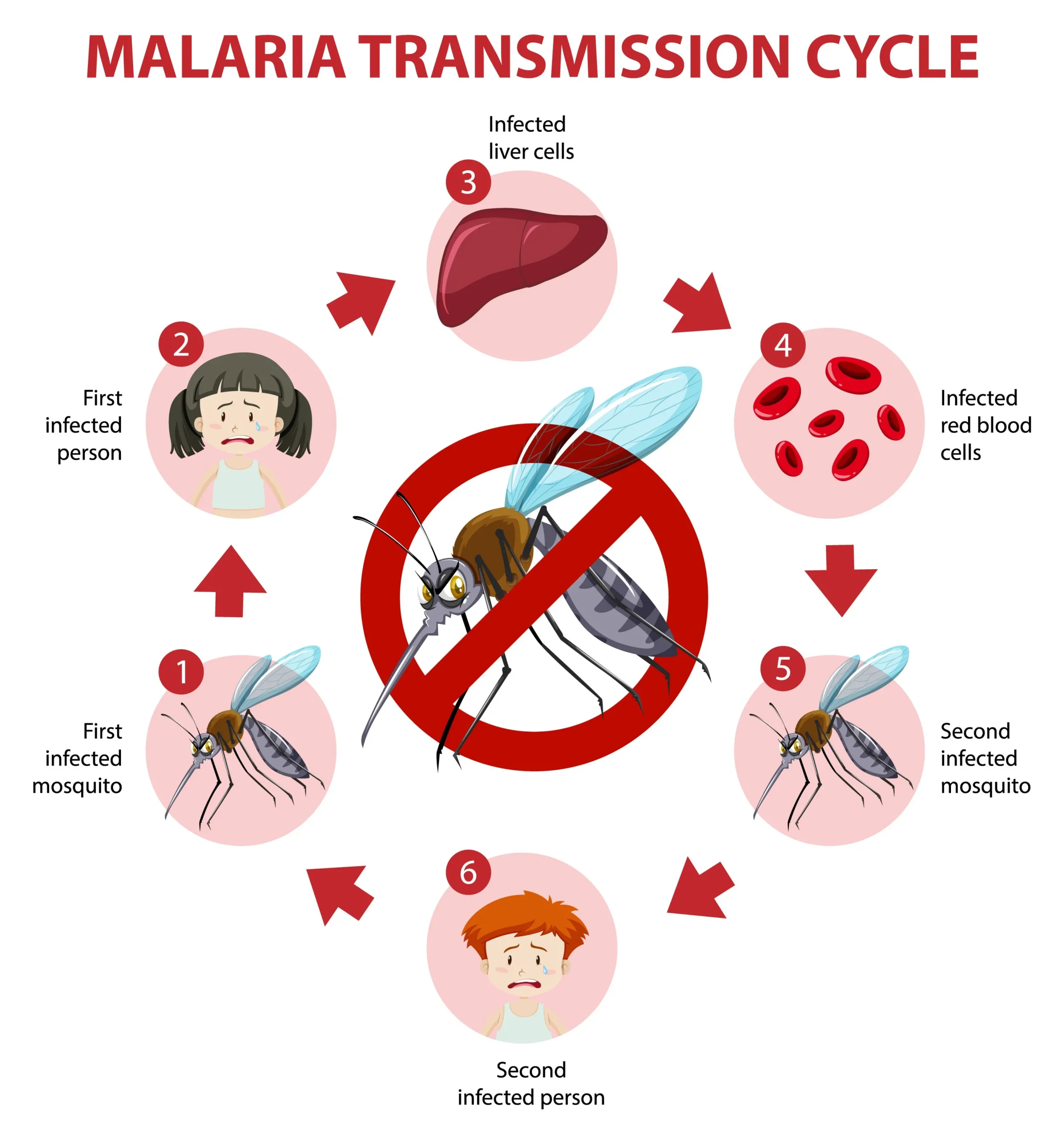
Malaria is caused by five different species of Plasmodium parasites: P. falciparum, P. vivax, P. ovale, P. malariae and P. knowlesi. The parasites are spread to people through the bites of infected female Anopheles mosquitoes which feed on human blood. In the human body, the parasites travel to the liver where they mature and reproduce before infecting and destroying red blood cells, leading to symptoms. Malaria transmission occurs mainly between dusk and dawn when the Anopheles mosquitoes are most active.
Risk Factors
Populations at highest risk include:
- Pregnant women
- Infants
- Children under 5 years old
- People with hiv/aids
- non-immune migrants and mobile populations
Pregnant women are vulnerable due to altered immunity making them more attractive to mosquitoes and more susceptible to infection. Children under 5 have little immunity and are highly susceptible to severe clinical disease. Other groups with a weakened immune system such as those with HIV/AIDS are more vulnerable to malaria.
Complications
If malaria is not promptly diagnosed and treated, it can lead to severe illness and life threatening complications including cerebral malaria, severe anemia, acute respiratory distress, and multiple organ failure. Pregnant women infected with malaria are at risk of low birth weight deliveries, miscarriage, stillbirths and neonatal death. Recurrent infections, particularly with P. falciparum, can result in severe malarial anemia. Untreated P. falciparum infections can progress rapidly to coma and death.
Diagnosis
Malaria diagnosis is challenging due to the non-specific nature of the symptoms which overlap with other febrile illnesses. The gold standard diagnostic test is microscopy examination of blood smears. Rapid diagnostic tests detecting malaria antigens can provide results within 20 minutes. Molecular techniques like polymerase chain reaction are also sometimes used. Diagnosis aims to identify the infecting Plasmodium species due to differences in severity, relapse patterns and drug resistance between species.
Procedures
If malaria is suspected, diagnosis should occur as quickly as possible either through microscopy or rapid diagnostic testing. Treatment is guided by test results indicating the infecting species, disease severity, region of acquisition and potential drug resistance patterns. Hospital admission is often required for severe cases or where oral treatment is contraindicated. Supportive care includes managing complications, preventing dehydration and malnutrition, and prophylaxis for related infections.
Treatment
Numerous antimalarial medications are available for treating uncomplicated malaria including: chloroquine, amodiaquine, quinine, mefloquine, lumefantrine, piperaquine, atovaquone-proguanil, tafenoquine, and artemisinin-based combination therapies like artemether-lumefantrine . Treatment selection considers Plasmodium species, disease severity, regional drug efficacy and resistance patterns. Severe cases require injectable artesunate or quinine and additional supportive clinical care. Note that some species can remain dormant in the liver causing relapse weeks or months after treatment completion.
Prevention
Malaria prevention aims to reduce mosquito bites and parasite transmission through insecticide treated mosquito nets, indoor residual spraying with insecticides, and antimalarial chemoprophylaxis drugs. Vector control methods like larviciding water bodies can suppress mosquito population density. Other strategies include educational campaigns promoting behaviors that minimize exposure to mosquitoes during peak biting times and drainage of stagnant water breeding sites. An experimental malaria vaccine (RTS,S) also shows modest efficacy and continues to be researched.
Research Advancements
With antimalarial drug resistance rising, intensive research is underway to develop new therapies, insecticides, diagnostics, vaccines and other tools. Existing drugs are being used in innovative dosing regimens and combinations to enhance efficacy. Genetic modification and bacterial infection are being trialed to reduce mosquito lifespans or fertility. Scientists are also exploring transmission blocking by targeting mosquito salivary proteins. With the rise of drug resistance, ongoing research and development is critical for discovering and delivering the next generation of malaria solutions.
In summary, malaria remains one of humanity’s greatest health challenges disproportionately affecting vulnerable groups like children and pregnant women. While preventable and treatable, drug resistance threatens progress made in reducing global malaria burden. Significant advancements continue to be made in developing and implementing evidence-based strategies and tools for effectively diagnosing, treating and preventing this life-threatening parasitic disease. Sustained political commitment and funding is vital for eliminating malaria which still claims hundreds of thousands of lives each year.